





Introduction
Despite being the globe’s third leading killer, the risk factors for Chronic Obstructive Pulmonary Disease (COPD) have long been a mystery. Aside from the genetic disorder alpha 1-antitrypsin deficiency, it has never fully been understood why some non-smokers develop diseases such as COPD, and yet lifelong smokers may not.
Thanks to the work of researchers in the study Human airway branch variation and chronic obstructive pulmonary disease[i], lead by Benjamin Smith, some light has been shed on this very topic. These researchers have discovered a previously unknown genetically-inherited risk factor for COPD. Their work has revealed that central airway branching variants can increase one’s risk of developing COPD and other respiratory illnesses and that an incredible 26.5% of the world’s population has one of these branching variants.
The Methodology
Smith and team examined Computed Tomography (CT) scans of 3,169 people in the Multi-Ethnic Study of Atherosclerosis (MESA) Lung Study[ii]. The mean age was 69, and 48% were male. The ethnic distribution among the participants was 39% Caucasian, 27% African-American, 21% Hispanic and 13% Asian-American. Fifty four percent were current or former smokers with a median exposure of 15 pack years.
Researchers also combined the data from MESA with results from the Subpopulations and Intermediate Outcome Measures in COPD Study, or SPIROMICS, to gather data from a pool of 3,363 participants, 1,212 of whom had been diagnosed with COPD.
Among the participants, airway branch variations were present in 26.5%, while 73.5% had standard airway anatomy (figure A). The most common variant (figure B) was seen in 16% of participants, and consisted of an accessory subsuperior airway. This variation was more common among Caucasians, and less common among Asian-Americans. The second most common, seen in 6%, was an absence of the right-medial basal airway (figure C). This variation was more common in Asian-Americans, and less among African-Americans. The remaining 4% of participants had rare branching variants.

Findings
When researchers compared the results of those with regular airway anatomy to those with branching variations, participants with variations were shown to have a higher risk of developing COPD.
When compared to those with normal airway anatomy, those with an accessory subsuperior airway had a 40% greater chance of developing COPD, regardless of whether or not they were smokers. Participants with an absent right-medial basal airway had a 55% greater chance of developing COPD if they were non-smokers, a risk that increased to 78% for smokers.
However, it was not just branching patterning that varied among participants. Both variations were found to have predictable changes throughout the entire lung, which researchers believe further contribute to the increased risk of disease development.
The most common branching variation, the accessory subsuperior airway, was found to have segment lengths that were 3.7% shorter than average throughout the entire lung, not just in the accessory lobe. The presence of an accessory subsuperior airway also demonstrated larger airspace in all lobes, and a higher number of central airway bifurcations.
While the variant which causes the absence of the right-medial basal airway was found to have segment lengths statistically similar to normal airway anatomy, the airway lumen throughout the lungs was found to be significantly narrower.
Associations between these branch variants and the likelihood of developing COPD did not differ by gender, race, ethnicity, presence of childhood asthma, second-hand smoke exposure, or maternal smoking during pregnancy.
Heritability
Because of the central positioning of these common variations, researchers hypothesized that their absence or presence did not change in adulthood. They compared CT scans from 300 MESA participants spanning a ten year interval, and there were no significant changes. This suggested to researchers that the branch variations did not occur in adulthood.
As the variants were found to be stable, researchers further hypothesized that these variations were indeed heritable. They selected 16 unrelated MESA participants with variant anatomy and conducted a CT scan on the participants’ siblings.
Among siblings, the presence of an accessory subsuperior airway was 46%; higher than the 16% prevalence among the general population. The absent right medial-basal airway was prevalent at a rate of 31% among siblings, also greater than the prevalence of 6% among the general population. Given these findings, the researchers further hypothesized these variations reflected differing function of the genes which regulate airway morphology.
Researchers conducted a targeted gene analysis of 109 single nucleotide polymorphisms (SNP) located on 11 genes. Two SNPs on chromosome 5 were associated with the absence of a right medial-basal airway. None of the selected SNPS were found to be associated with the presence of an accessory subsuperior airway.
Discussion
One’s central airway is essential for the removal of harmful particulate matter. Anything that impedes the removal of inhaled debris may lead to an increased likelihood of disease development and interstitial damage. Prior to the conduction of this study, it was unlikely many people would have thought of the anatomy of the central airways when considering risk factors for pulmonary diseases.
Smith and team believe that the increase in COPD risk among these lung variations is not due to the branching pattern themselves, but because of the associated changes that were found to accompany them. The increase in the amount of central airway bifurcations in the accessory subsuperior airway creates an increase in area for sedimentation of particulate matter. The narrower airway lumen associated with the absence of the right-medial basal airway greatly affects airway resistance. All of these changes lead to a decreased ability to clear harmful matter from one’s lungs.
These findings suggest that airway branch variations, which are common and easily identifiable, reflect widely altered lung structure and provide a genetically determined basis for COPD susceptibility, even among those who do not smoke. Smith and team are hopeful that in the future preventative and therapeutic interventions, based on the presence of abnormal lung morphologies, may one day improve patient outcomes.
Though the best way to prevent one’s chances of developing COPD is still to abstain from or quit smoking, perhaps one day in the future healthcare practitioners will be able to warn patients that this risk factor for COPD runs in their family, and to choose their habits accordingly.
[i] Smith BM et al. Human airway branch variation and chronic obstructive pulmonary disease. Proceedings of the National Academy of Sciences of the United States of America E (2018): 974-981.
[ii] Smith BM, et al. The Multi-Ethnic Study of Atherosclerosis (MESA) COPD Study and the Subpopulations and Intermediate Outcomes in COPD Study (SPIROMICS) Comparison of spatially matched airways reveals thinner airway walls in COPD. Thorax. 2014;69:987–996. [PMC free article] [PubMed]
Submitted by: by Tammy Drape, RRT
British Lung Foundation (England and Wales). VAT 648 8121 18
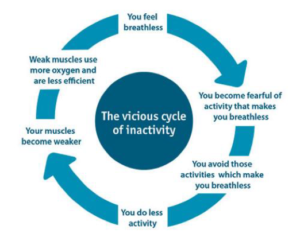
Having been an RRT for over 20 years, far too often I’ve seen patients discharged from hospital on oxygen, only to become socially isolated, less active or even sedentary, progressing to even more shortness of breath…and ultimately fall into the vicious cycle that often occurs with lung disease. They often feel like they’re alone.
 For every client that goes home on oxygen with CPR, we provide breathing techniques, strategies for coping with shortness of breath, and disease specific information. We also express the importance of staying active and understanding the downward spiral that they can easily fall into. Even further, we assess each of our clients to see if they may be good candidates for our “Community Pulmonary Rehabilitation program” or our “In Home Pulmonary Rehabilitation program.” By providing even the basics, we are able to influence the vicious cycle.
For every client that goes home on oxygen with CPR, we provide breathing techniques, strategies for coping with shortness of breath, and disease specific information. We also express the importance of staying active and understanding the downward spiral that they can easily fall into. Even further, we assess each of our clients to see if they may be good candidates for our “Community Pulmonary Rehabilitation program” or our “In Home Pulmonary Rehabilitation program.” By providing even the basics, we are able to influence the vicious cycle.
Who are we?
Centre for Pulmonary Rehabilitation (CPR) was established June of 2005 by Tammy Draper (Registered Respiratory Therapist) with over 20 year experience in pulmonary rehabilitation. CPR is unique in providing pulmonary rehabilitation and follows American Association of Cardiovascular Pulmonary Rehab Guidelines. Initially launched as a pulmonary rehab only, we soon realized patients who needed pulmonary rehab the most couldn’t afford it as the cost is approx. $2,200 per patient to run rehab for eight weeks, including all assessments and educational material. In an attempt to help decrease the cost of the pulmonary rehab, we accessed the “Prism” Program funded by Glaxo Smith Kline and Pfizer, however, this was only for a two year period. We had to come up with a solution so that we could reach all patients in need.
CPR’s business model is unique in the health care industry. CPR’s goal has been to “invest back into our community” by providing FREE pulmonary rehabilitation to those in need, while following best practices. Our solution: we became a Home Oxygen Vendor and a CPAP vendor. We reinvest proceeds from other revenue streams (home oxygen and CPAP/sleep therapy) into the pulmonary rehabilitation program, making it free. For the past nine years, pulmonary rehab has been free for all clients in need. Our business model has enabled us to help more patients in our community and provide the highest level of care possible. Without the support of home oxygen and CPAP referrals, we would not be able to provide this service.
A recent survey was conducted (Pulmonary Rehabilitation in Ontario: A Cross-Sectional Survey, March 2015 Ontario Health Technology Assessment Series; Vol. 15: No. 8, pp. 1–67, March 2015)
- The survey showed that the province has relatively few program spaces compared to the number of people who could use them.
- More than 700,000 people in Ontario have chronic lung disease.
- The facilities currently available in this province can support only about 1.12% of the people who could potentially benefit from pulmonary rehabilitation.
The Pulmonary Rehab Program includes: individual exercise assessment for improved endurance, improve strength to do daily activities, education on use of medications, disease specific patient and family education, active physician monitoring and intervention, breathing retaining, physical support, promote independence, smoking cessation counseling and motivation to continue maintenance.
Program Goals: Improve quality of life, reduce respiratory symptoms and exacerbations, increase knowledge of lung disorders, return to work or leisure activities, improve performance of aids to daily living and become an expert in their own care.
Quality Control (Measures Key Performance Indicators (KPIs): CPR has rigorous KPIs that are recorded and reported in a summary to each referring physician when a client graduates from our pulmonary rehabilitation program. KPIs include; six minute walk test, St. Georges Quality of Life Questionnaire and customer satisfaction survey.
What are the “best practices”?
Best Practices for treatment of COPD
- Quality Based Procedures: COPD

Quality-Based Procedures: Clinical Handbook for Chronic Obstructive Pulmonary Disease, Health Quality Ontario & Ministry of Health and Long-Term Care, January 2013,
- Canadian Thoracic Society: COPD
Actual Recommended



